Silajathu Rasayana in management of Ankylosing Spondylitis - A Case Report
Hariharan Mk1*, Giri PV2
DOI:10.21760/jaims.9.11.50
1* Hariharan Mk, Post Graduate Scholar, Dept of Kayachikitsa, Vaidyaratnam Ayurveda College Ollur, Thrissur, Kerala, India.
2 Giri PV, Professor, Dept of Kayachikitsa, Vaidyaratnam Ayurveda College Ollur, Thrissur, Kerala, India.
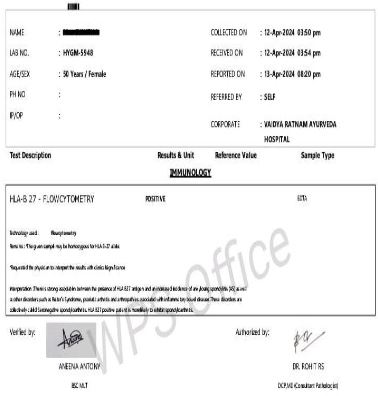
Ankylosing Spondylitis is a chronic seronegative inflammatory condition that primarily impacts the sacroiliac joint and spine, potentially leading to the fusion of spinal bones. The exact cause of this condition remains unknown. A 50 year old female patient was admitted to the Kayachikitsa inpatient department of Vaidyaratnam Ayurveda College, Ollur, presenting with both knee pain and swelling, pain in both elbow joints, and generalized back pain. She was treated by following the Amavatha management protocol, which included internal administration of Ayurvedic formulations such as Amrithotharam Kashaya, Indukantham Kashaya, Yogaraja Guggulu, Punarnavasam, and Rasnapanchakam Kashaya. External therapies such as Churna Pinda Sweda, Snehapana, Sarvanga Taila Dhara and Virechana. Silajathu Rasayana were administered in the final stage of the treatment. After six weeks of treatment, the patient experienced significant relief from upper and lower back pain, reduced elbow pain, and noticeable improvement in knee joint swelling and discomfort. This case study emphasizes the efficacy of Ayurvedic management especially Rasayana chikitsa in achieving substantial symptom improvement within a short duration.
Keywords: Ankylosing spondylitis, Rasayana therapy, Silajathu Rasayana, Amavata, Case report
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Post Graduate Scholar, Dept of Kayachikitsa, Vaidyaratnam Ayurveda College Ollur, Thrissur, Kerala, India. Email:  |
Hariharan Mk, Giri PV, Silajathu Rasayana in management of Ankylosing Spondylitis - A Case Report. J Ayu Int Med Sci. 2024;9(11):336-342. Available From https://jaims.in/jaims/article/view/3861 |
 |
 ©
©