Transdermal Drug Delivery System: A Review of Current Advances and Challenges
Chankhore SA1*, Gawande VK2, Mhaske SD3, Wagh RG4, Sharma TJ5
DOI:4048
1* Sanjivani A Chankhore, Pharmacy Student, Dept of Pharmaceutical Sciences, Satyajeet College of Pharmacy Mehkar, Buldana, Maharashtra, India.
2 Vikas K Gawande, Assistant Professor, Dept of Pharmaceutical Sciences, Satyajeet College of Pharmacy Mehkar, Buldana, Maharashtra, India.
3 Shivshankar D Mhaske, Principal, Dept of Pharmaceutical Sciences, Satyajeet College of Pharmacy Mehkar, Buldana, Maharashtra, India.
4 Rutuja G Wagh, Pharmacy Student, Dept of Pharmaceutical Sciences, Satyajeet College of Pharmacy Mehkar, Buldana, Maharashtra, India.
5 Tejas J Sharma, Assistant Professor, Dept of Pharmaceutical Sciences, Satyajeet College of Pharmacy Mehkar, Buldana, Maharashtra, India.
Recently, various non-invasive administrations have emerged as alternatives to traditional needle injections. A Transdermal drug delivery system (TDDS) is the most attractive of these due to its low Rejection rate, excellent ease of administration, and superb convenience and persistence among patients. TDDS Could be applicable not only in pharmaceuticals but also in the skin care industry, which includes cosmetics. Since this This method mainly involves local administration. The skin infusion enhancer technique has been advanced to improve the bioavailability of the drugs. So various Transdermal dosage forms have been prepared like: Transdermal patches, Gel, Cream, Ointments, etc. The Transdermal route is a viable option to enhance the variety of drugs. Transdermal drug delivery has become the primary route of delivery for a variety of medications that would otherwise be difficult to supply. There are some Advantages to Transdermal medicine administration. Mainly to avoid first-pass metabolism and a stomach Environment that would make the drug ineffective in drugs prescribed for skin-related problems and for systemic Effects in curing other organs’ diseases. Hormone replacement therapy, pain relief, smoking withdrawal, Neurological disorders and angina pectoris such as Parkinson’s disease are all under the categories of Transdermal products and Applications. Formulated to release the drug into systemic circulation at the optimal rate, it must be retained in Skin for the required period without inducing sensitization or irritation of the skin. Avoiding first-pass metabolism to achieve Bioavailability with minimal peaks and troughs, Tolerance and dose are being achieved. In the case of Continuous Delivery, maintaining high compliance of the patients is required.
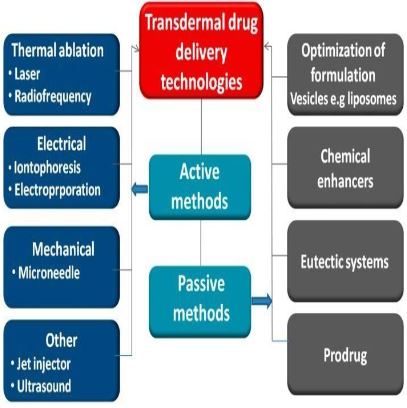
Keywords: Transdermal drug delivery system, physical and chemical method, challenges
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Pharmacy Student, Dept of Pharmaceutical Sciences, Satyajeet College of Pharmacy Mehkar, Buldana, Maharashtra, India. Email:  |
Chankhore SA, Gawande VK, Mhaske SD, Wagh RG, Sharma TJ, Transdermal Drug Delivery System: A Review of Current Advances and Challenges. J Ayu Int Med Sci. 2024;9(11):203-212. Available From https://jaims.in/jaims/article/view/4048 |
 |
 ©
©